
A cavity is a permanently damaged area in the hard surface of your tooth that develops into a tiny opening or hole. Cavities form when bacteria in your mouth produce acids that erode tooth enamel, and you need professional treatment to stop the damage from spreading deeper into the tooth structure.
At BrightSmile Dental Clinic in Putalisadak, we see patients every week who ignored early cavity symptoms until pain forced them to seek treatment. This article explains how to recognize cavity signs early, understand your filling options, and choose the right treatment for your specific situation in Kathmandu.
Cavity Symptoms: How to Know You Might Need a Tooth Filling

Recognizing cavity symptoms early saves you from more complex and expensive treatments later. The challenge is that early cavities rarely hurt, so you must watch for subtle warning signs that decay has started.
Early cavity signs (white spots, mild sensitivity, rough edges)
The first sign of a cavity is often a white or chalky spot on your tooth surface. This white spot indicates mineral loss in the enamel, the earliest stage of decay that you can sometimes reverse with proper fluoride treatment and improved oral hygiene.
You might feel mild sensitivity when you consume sweet foods or cold drinks. The tooth enamel has weakened enough that temperature and sugar can reach the more sensitive layer beneath. Your tongue may detect a rough edge or small pit where the enamel surface has broken down, even before you can see visible discoloration.
Many patients dismiss these early signs, assuming sensitivity will fade on its own. It rarely does. The white spot will darken to yellow or brown as decay progresses, and the rough area will enlarge into an actual hole you can feel with your tongue or see in the mirror.
Symptoms of deeper decay (sharp pain, lingering cold/heat sensitivity)
Sharp, stabbing pain when you bite down on a tooth signals that decay has reached the dentin layer beneath your enamel. Dentin contains tiny tubules that connect directly to the tooth nerve, so pressure from chewing compresses these tubules and triggers pain.
Temperature sensitivity that lingers for 10 to 30 seconds after you remove the hot or cold stimulus indicates deeper decay. Healthy teeth stop hurting within 2 to 3 seconds after you remove the trigger. Prolonged sensitivity means the cavity has penetrated close to the nerve chamber, and bacteria may be causing inflammation inside the tooth.
You may notice a persistent dull ache that worsens at night when you lie down. This happens because increased blood flow to your head raises pressure inside the tooth, and the inflamed nerve has no room to expand. Some patients describe a throbbing sensation that keeps them awake or forces them to sleep sitting up.
Visible holes, brown or black stains, or pieces of tooth breaking off during meals are unmistakable signs of advanced decay. The bacteria have destroyed so much tooth structure that the remaining enamel collapses under normal chewing forces.
Cavities between teeth: why they’re easy to miss
Interproximal cavities (cavities between teeth) cause no visible symptoms until they grow large enough to break through the tooth surface. You cannot see these cavities in a mirror, and they develop in the tight contact area where your toothbrush cannot reach effectively.
Food constantly packs between your teeth, creating an ideal environment for bacteria. The first symptom you notice is food trapping in a space where it never trapped before, or dental floss shredding or catching on a rough spot. You might feel a sharp edge with your tongue when you run it along the side of a tooth.
Persistent bad breath or a foul taste in one area of your mouth can indicate a cavity between teeth. The decayed tooth structure harbors bacteria that produce sulfur compounds, creating an odor that brushing and rinsing do not eliminate.
X-rays are the only reliable way to detect interproximal cavities early. We see patients at BrightSmile who developed cavities large enough to require crowns instead of simple fillings, purely because they skipped regular dental exams and X-rays for 3 to 4 years.
When tooth pain is NOT a cavity (stain, gum recession, crack, sinus pressure)
Not every tooth sensitivity or discoloration means you have a cavity. External stains from tea, coffee, or tobacco often darken teeth without causing actual decay. You can remove surface stains during a professional cleaning, whereas cavities require drilling and filling.
Gum recession exposes the tooth root surface, which lacks protective enamel and feels sensitive to cold, heat, and brushing. The root surface appears yellowish, and the sensitivity is usually widespread across multiple teeth rather than localized to one spot. Desensitizing toothpaste and fluoride treatment often resolve this sensitivity without fillings.
Cracked teeth cause sharp pain when you bite down, similar to cavity pain, but the pain stops immediately when you release pressure. Cracks typically result from grinding your teeth at night, chewing hard objects, or trauma. You need a different treatment approach (bonding, crown, or in severe cases, extraction) rather than a filling.
Sinus infections create pressure in your upper back teeth because the tooth roots sit directly beneath the sinus cavity. You feel a dull ache across multiple upper teeth on one side, worsening when you bend forward or lie down. The pain resolves when the sinus infection clears, and you do not need dental treatment.
Diagnosis: How Dentists Confirm a Cavity Before Filling

Professional diagnosis prevents unnecessary treatment and ensures you receive the right intervention at the right time. We use multiple diagnostic tools at BrightSmile to assess cavity depth, location, and severity before recommending treatment.
Dental exam and X-ray: what they detect and why it matters
A visual exam detects surface cavities, but X-rays reveal hidden decay between teeth, beneath old fillings, and in the early stages before visible holes form. Your dentist uses a small mirror and explorer tool to check each tooth surface for sticky spots, rough areas, and discolored patches that indicate decay.
Bitewing X-rays (the small films you bite down on) show the tooth crowns and the bone level between teeth. These X-rays detect interproximal cavities, secondary decay under existing fillings, and bone loss from gum disease. Periapical X-rays (the larger films placed behind individual teeth) show the entire tooth from crown to root tip, revealing deep decay near the nerve and infections at the root end.
Digital X-rays reduce radiation exposure by 70 to 80 percent compared to traditional film X-rays, and we can enhance the image on a computer screen to show you exactly where decay exists. You should have bitewing X-rays every 12 to 24 months if you have a history of cavities, or every 24 to 36 months if your oral health is excellent.
The exam also includes checking for loose fillings, cracked teeth, gum inflammation, and oral cancer lesions. Many patients discover multiple issues during one appointment, allowing us to create a comprehensive treatment plan rather than addressing problems piecemeal.
Cavity stages (enamel → dentin → near nerve) and treatment options at each stage
Cavities progress through 5 distinct stages, and the treatment complexity increases with each stage.
- Stage 1 involves enamel demineralization (white spot lesions) that you can reverse with fluoride therapy, improved brushing, and dietary changes, no filling required.
- Stage 2 occurs when the cavity breaks through the enamel into the dentin layer. The tooth becomes sensitive, and you need a filling to remove the decay and seal the hole. Composite or amalgam fillings work well at this stage.
- Stage 3 happens when decay reaches the inner third of dentin, close to the nerve chamber. You may experience moderate to severe pain, and the filling may require a protective liner or base material to insulate the nerve. Some teeth at this stage need root canal treatment (RCT) if the nerve becomes inflamed.
- Stage 4 involves pulp (nerve) damage, causing intense pain, abscess formation, or swelling. You need RCT to remove the infected nerve tissue, followed by a crown to restore the tooth structure. Simple fillings do not work at this stage.
- Stage 5 is tooth destruction, where so much structure is lost that the tooth cannot be saved. Extraction becomes necessary, followed by an implant, bridge, or partial denture to replace the missing tooth.
Early detection at Stage 1 or 2 saves you from painful and expensive treatments later. Regular dental visits every 6 months allow us to catch cavities when they are small and simple to treat.
When you may not need a filling yet (remineralization and monitoring)
Incipient caries (very early cavities confined to enamel) can heal through a process called remineralization. Your saliva contains calcium and phosphate ions that can rebuild weakened enamel if you reduce acid exposure and increase fluoride use.
We monitor these early lesions with photographs and periodic X-rays to confirm the decay is not progressing. You must commit to excellent oral hygiene, fluoride toothpaste twice daily, fluoride mouth rinse, and dietary changes (reducing sugary snacks and acidic drinks). Some patients benefit from prescription-strength fluoride gel applied at home.
This conservative approach works only for enamel-limited cavities that have not penetrated into dentin. The moment the cavity enters dentin, bacteria colonize the tooth and create an environment where remineralization cannot occur. You must have the decay removed and the tooth filled.
Children and adolescents often respond better to remineralization therapy than adults do, because young enamel is more porous and absorbs fluoride more readily. However, compliance with oral hygiene instructions is critical, missing fluoride applications or continuing sugary snacks will cause the cavity to progress rapidly.
At BrightSmile, we provide written instructions for remineralization therapy and schedule follow-up visits every 3 to 4 months to monitor progress. Approximately 30 to 40 percent of early lesions stabilize or reverse with this approach, sparing patients from unnecessary drilling.
Deep cavities: conservative decay removal to protect the nerve
Selective carious tissue removal (also called conservative or minimally invasive dentistry) preserves healthy tooth structure and protects the nerve in deep cavities. Traditional cavity preparation removed all softened dentin, sometimes exposing the nerve and requiring RCT.
Modern techniques remove only the infected outer layer of decay, leaving a thin layer of affected but remineralizable dentin near the nerve. The dentist applies a protective liner (calcium hydroxide or glass ionomer) over this layer, then places the final filling material on top. The preserved dentin acts as a thermal and bacterial barrier, and the tooth often heals without nerve damage.
This approach is particularly valuable in young patients whose nerve chambers are large and close to the tooth surface. You avoid RCT in many cases, though you must return for follow-up visits to ensure the tooth remains asymptomatic.
Some dentists use stepwise excavation, removing decay in two appointments separated by 6 to 12 months. The first visit removes the bulk of decay and places a temporary filling, allowing the dentin to remineralize. The second visit removes any remaining soft tissue and places the final restoration.
Conservative decay removal requires precise technique and high-quality bonding materials. Not all cavities are suitable for this approach, teeth with irreversible pulpitis (severe nerve inflammation) or abscess still need RCT.
Best Filling Type: A Clear Comparison (What Works Best for Your Tooth)
Filling materials vary in strength, appearance, cost, and longevity. The “best” filling depends on the tooth location, cavity size, your bite force, aesthetic concerns, and budget. This section explains each material’s strengths and limitations so you can make an informed choice.
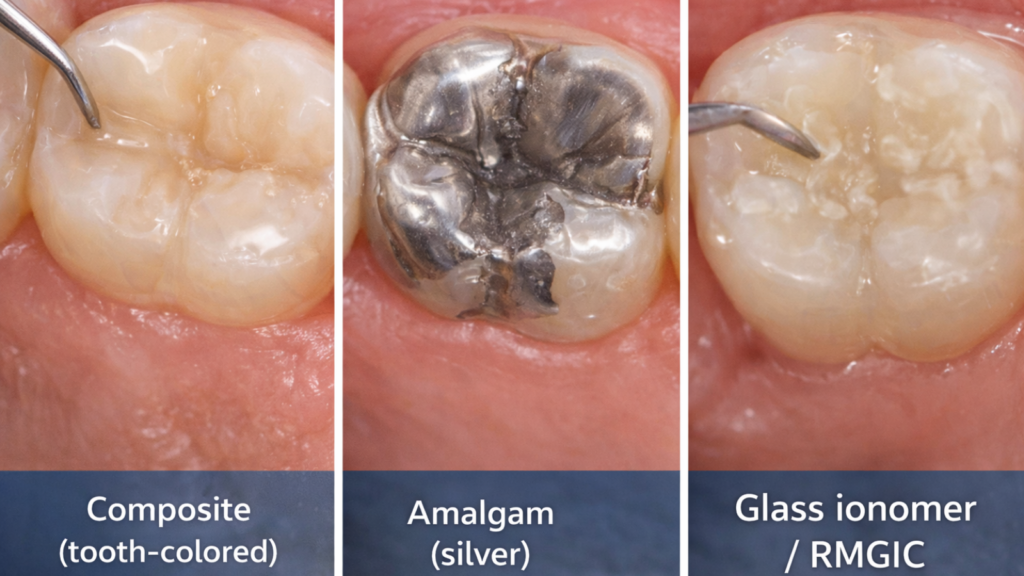
1. Composite (tooth-colored) fillings: best uses, pros/cons, and durability
Composite resin fillings bond chemically to tooth structure, allowing for conservative cavity preparation and excellent aesthetics. The material comes in multiple shades that match your natural tooth color, making it the standard choice for front teeth and visible back teeth.
Composite fillings are placed in layers and hardened with a blue curing light. The layering technique allows the material to adapt to cavity shape, creates a strong bond, and minimizes shrinkage stress. The entire process takes 30 to 60 minutes per tooth, longer than amalgam placement.
The main advantage is tooth conservation, composite bonds to enamel and dentin, so the dentist removes only the decayed portion without cutting away healthy structure. The filling also insulates the tooth from temperature changes better than metal, reducing post-operative sensitivity in many cases.
Composite fillings last 5 to 10 years on average, though longevity depends on cavity size, tooth location, and your oral habits. Large composite fillings in molars (especially if you grind your teeth) may chip or fracture sooner than amalgam fillings. The material absorbs stains from coffee, tea, and curry over time, and polishing during cleanings helps maintain the appearance.
Cost in Kathmandu ranges from NPR 2,000 to NPR 6,000 per tooth, depending on cavity size and clinic location. BrightSmile uses high-quality composite systems that resist wear and maintain color stability better than economy brands.
2. Amalgam (silver) fillings: strength, cost, and common safety concerns
Amalgam is a mixture of silver, tin, copper, and mercury that hardens into an extremely durable filling material. It has been used for over 150 years and remains the strongest option for large cavities in back teeth that endure heavy chewing forces.
The main advantage of amalgam is longevity, these fillings last 10 to 15 years or longer with proper care. The material is less technique-sensitive than composite, meaning it tolerates moisture during placement and requires less precision in bonding. Amalgam costs 20 to 30 percent less than composite, making it the most economical choice for large restorations.
The disadvantage is appearance, silver fillings are visible when you smile or laugh. Amalgam also requires more aggressive cavity preparation because it does not bond to tooth structure, so the dentist must create mechanical retention by cutting undercuts into the tooth. This removes more healthy enamel and dentin than composite preparation does.
Mercury safety concerns have been extensively studied. The World Health Organization (WHO), American Dental Association (ADA), and Nepal Medical Council all state that amalgam is safe for adults and children over age 6. The mercury in amalgam binds to the other metals and releases only trace vapor amounts, far below harmful levels. We do not recommend amalgam for pregnant women, nursing mothers, or people with kidney disease as a precautionary measure.
Amalgam use is declining worldwide due to aesthetic preferences and environmental concerns (mercury disposal), but it remains a valid option for patients who prioritize strength and cost over appearance.
3. Glass ionomer / RMGIC: fluoride benefit, best cases (kids/gumline), and limitations
Glass ionomer cement (GIC) and resin-modified glass ionomer cement (RMGIC) release fluoride over time, helping prevent recurrent decay around the filling margins. These materials bond chemically to dentin without acid etching, making them useful in high-moisture environments like gumline cavities.
GIC is weaker than composite and amalgam, so we use it primarily for small cavities in baby teeth, gumline (cervical) cavities in adults, and temporary fillings. The material sets through a chemical reaction and does not require a curing light, allowing faster placement in uncooperative children or patients with limited mouth opening.
RMGIC contains resin components that improve strength and wear resistance compared to traditional GIC. We use RMGIC as a base layer under composite fillings in deep cavities, taking advantage of the fluoride release and excellent sealing properties.
The main limitation is aesthetics, GIC and RMGIC do not match tooth color as closely as composite, and the surface tends to wear faster. These materials last 3 to 5 years on average, shorter than composite or amalgam. We typically replace GIC fillings with composite or amalgam once the tooth is fully erupted and the patient can tolerate longer appointments.
Costs range from NPR 1,500 to NPR 3,500 per tooth, slightly less than composite. BrightSmile uses high-strength RMGIC formulations that extend the lifespan and improve aesthetics compared to conventional GIC.
Direct filling vs indirect inlay/onlay: when “best filling” becomes an onlay or crown
Direct fillings (composite, amalgam, GIC) are placed and shaped inside your mouth during a single appointment. Indirect restorations (inlays, onlays, crowns) are fabricated in a dental laboratory or milled by a chairside CAD/CAM system, then cemented onto the tooth in a second appointment.
You need an indirect restoration when the cavity is so large that a direct filling would fracture under chewing forces. The general rule is that any filling replacing more than 50 percent of the distance between the tooth cusps (the pointed parts of molars) should be an onlay or crown. These restorations cover and protect the remaining tooth structure, distributing bite forces evenly and preventing cracks.
Inlays fit inside the cusps, similar to a large filling. Onlays extend over one or more cusps, providing greater protection. Full crowns cover the entire tooth and are necessary when multiple cusps are broken or when the tooth has had RCT.
Indirect restorations are stronger and last longer than direct fillings (10 to 20 years for porcelain or gold onlays), but they cost significantly more. Porcelain inlay/onlay costs range from NPR 15,000 to NPR 35,000 per tooth in Kathmandu, compared to NPR 2,000 to NPR 6,000 for a composite filling.
The decision depends on the amount of remaining tooth structure, the location of the tooth, and your budget. At BrightSmile, we show you the cavity size on X-rays and photographs, explain both options, and let you choose based on your priorities. Many patients start with a composite filling and accept that it may need replacement in 5 to 7 years, while others prefer the onlay investment for long-term durability.
Choosing the Right Filling: Decision Guide by Tooth Location, Bite, and Budget

This section provides a practical framework for selecting the most appropriate filling material based on your specific situation. Use these guidelines in consultation with your dentist to make a confident decision.
Best filling for molars vs front teeth vs gumline vs between teeth
Front teeth (incisors and canines) should always receive composite fillings for aesthetic reasons. These teeth are visible when you smile, and silver fillings would stand out noticeably. Composite also preserves tooth structure because front teeth have thin enamel and large nerve chambers, so conservative preparation is critical.
Molars (back teeth) can receive either composite or amalgam, depending on cavity size and your preferences. Small to medium molars cavities (one or two surfaces) work well with composite, especially in patients who prefer tooth-colored restorations. Large molar cavities involving three or more surfaces perform better with amalgam due to superior wear resistance, or with onlays if you want both strength and aesthetics.
Gumline cavities (cervical caries) occur at the junction of tooth and gum, often in patients with gum recession or aggressive brushing. Composite is the standard choice because it bonds well to exposed root surfaces and matches the tooth color. RMGIC is an alternative in patients with poor moisture control or ongoing decay risk, thanks to fluoride release.
Cavities between teeth (interproximal) require careful material selection. Composite works well for small to medium interproximal cavities, but the dentist must use a matrix band (a thin metal strip) to recreate the contact point between teeth. Improper technique leaves a gap where food packs, causing inflammation and discomfort. Amalgam is less technique-sensitive for contact recreation but shows a dark shadow through the tooth enamel that some patients find unaesthetic.
Best filling if you grind your teeth (bruxism) or have a strong bite
Patients with bruxism (teeth grinding) or heavy bite forces need the most durable filling materials to prevent fractures. Composite fillings in molars may chip or crack within 2 to 3 years in severe grinders, whereas amalgam or gold can last 10 to 15 years.
You should address the underlying bruxism with a night guard (occlusal splint) to protect both the fillings and the natural teeth. A custom night guard costs NPR 8,000 to NPR 15,000 in Kathmandu and extends the life of all dental restorations by reducing grinding forces.
Porcelain or zirconia onlays and crowns are the best long-term solution for large cavities in bruxism patients. These materials resist wear better than composite and distribute forces across the entire tooth, preventing cracks. The higher upfront cost (NPR 15,000 to NPR 45,000 per tooth) is often offset by the extended lifespan and reduced need for replacements.
Some patients benefit from composite reinforced with fiber posts or internal bracing, though this technique is not widely available in Nepal. Standard composite remains acceptable for front teeth and small back teeth cavities, even in grinders, because these teeth experience less force than molars.
Best filling for large cavities: when composite is not enough
Composite fillings perform poorly in very large cavities because the material shrinks slightly during curing, creating stress at the margins. This stress can cause cracks in the surrounding tooth structure, post-operative sensitivity, and early failure.
The critical threshold is cavity depth and width. Cavities deeper than 4 to 5 millimeters (mm) or wider than half the distance between cusps exceed the ideal range for composite. You should consider an indirect restoration (onlay or crown) or use amalgam if aesthetics are not a priority.
Layering techniques improve composite performance in larger cavities. The dentist places the material in 2 mm increments, curing each layer separately, which reduces total shrinkage stress. High-quality composite systems with low shrinkage formulations also help, though these materials cost more and are not always available in budget clinics.
Another option is a hybrid approach, using RMGIC as a base to replace lost dentin, then placing composite over the top for aesthetics and strength. This technique reduces the composite volume, minimizes shrinkage, and adds fluoride protection near the nerve.
You should always ask your dentist to explain why they recommend a particular material for large cavities. At BrightSmile, we use intraoral cameras and X-rays to show you the cavity dimensions and discuss the pros and cons of each option before you commit.
A simple “best filling type” checklist (aesthetics, longevity, sensitivity, cost)
Use this 4-factor checklist to guide your filling choice:
- Firstly, aesthetics: choose composite for all visible teeth (front teeth, premolars, upper molars that show when you smile). Choose amalgam, gold, or porcelain for non-visible back teeth if you prioritize strength over appearance.
- Secondly, longevity: choose amalgam, gold, or porcelain onlay for large cavities and heavy chewing forces. Choose composite for small to medium cavities in front teeth and premolars. Choose RMGIC only for temporary situations or baby teeth.
- Thirdly, sensitivity: choose composite or RMGIC if you have a history of severe sensitivity, as these materials insulate better than amalgam. Choose amalgam with a protective liner if you need strength but are concerned about temperature sensitivity.
- Fourthly, cost: choose amalgam for the lowest cost per tooth (NPR 1,500 to NPR 3,000). Choose composite for moderate cost and good aesthetics (NPR 2,000 to NPR 6,000). Choose onlay or crown for the highest upfront cost but longest lifespan (NPR 15,000 to NPR 45,000).
Discuss your priorities with your dentist. Some patients value aesthetics above all else and accept shorter composite lifespans. Others prioritize durability and choose amalgam despite the appearance. There is no universally “best” filling, only the best choice for your specific tooth, budget, and preferences.
The Tooth Filling Procedure and Aftercare: What to Expect and What’s Normal
Understanding the filling procedure reduces anxiety and helps you prepare for the appointment. This section explains each step and clarifies what sensations are normal versus warning signs that require follow-up.
Step-by-step: numbing, decay removal, bonding, shaping, polishing
The filling procedure begins with local anesthesia to numb the tooth and surrounding gum tissue. Your dentist applies topical anesthetic gel to the injection site, then slowly injects local anesthetic near the tooth nerve. You feel pressure and sometimes a brief stinging sensation, but the area becomes numb within 3 to 5 minutes.
Once numb, the dentist uses a dental drill (high-speed handpiece) to remove the decayed tooth structure. You hear a high-pitched whining sound and feel vibration, but you should not feel pain. Some patients describe a sensation of pressure or cold water spray, which is normal. The dentist removes all softened, discolored dentin and creates a clean cavity preparation.
For composite fillings, the tooth must be completely dry. The dentist places a rubber dam (a thin rubber sheet that isolates the tooth) or uses cotton rolls and suction to keep saliva away. Moisture contamination during bonding causes early failure. Next, the dentist applies acid etch to the enamel and dentin for 15 to 30 seconds, rinses thoroughly, and applies bonding agent. The bonding agent is cured with a blue LED light for 10 to 20 seconds.
Composite resin is placed in layers, each layer shaped to recreate the natural tooth anatomy and cured for 20 to 40 seconds. The dentist builds up the filling until it slightly overfills the cavity, then uses finishing burs and polishing discs to shape and smooth the surface. You bite down on articulating paper (thin colored paper) so the dentist can identify high spots and adjust the filling until your bite feels even.
The final step is polishing with fine abrasive paste to create a smooth, glossy surface that resists staining. The entire procedure takes 30 to 90 minutes, depending on cavity size and material choice. Amalgam placement is faster because it does not require bonding or layering.
Does a filling hurt? what you’ll feel during and right after treatment
You should feel no pain during the procedure if the anesthesia is effective. Some patients report pressure, vibration, or odd sounds, but these sensations are not painful. The dentist can add more anesthetic at any time if you feel discomfort.
After the anesthesia wears off (2 to 4 hours), you may experience mild soreness in the gum tissue where the injection was placed. This resolves within 24 hours. The tooth itself may feel sensitive to cold, heat, or biting for 3 to 7 days as it adjusts to the new filling. This is normal, especially for deep cavities close to the nerve.
Sharp pain when you bite down immediately after the filling suggests a high spot (the filling is too tall and hits the opposing tooth before your other teeth make contact). Contact your dentist for a simple adjustment, this takes 5 minutes and resolves the pain instantly.
Throbbing pain or extreme sensitivity that worsens over the first few days indicates possible nerve inflammation (pulpitis). Deep cavities sometimes irritate the nerve despite conservative treatment, and the tooth may require root canal therapy. This occurs in approximately 5 to 10 percent of deep fillings.
Most patients return to normal eating and function within 24 to 48 hours. Sensitivity that persists beyond 2 weeks should be evaluated, as it may indicate incomplete decay removal, a crack in the tooth, or bonding failure.
When you can eat after a filling (same-day do’s and don’ts)
You can eat soft foods on the opposite side of your mouth as soon as the anesthesia wears off. Eating while numb is dangerous because you can bite your lip, cheek, or tongue without feeling it, causing painful wounds that take days to heal.
Composite fillings harden instantly under the curing light, so there is no waiting period for the material to set. You can technically eat immediately after leaving the dental office, though it is safer to wait until sensation returns fully.
Amalgam fillings take 24 hours to reach full strength, so you should avoid chewing hard or sticky foods on the filled tooth for the first day. Soft foods (yogurt, soup, mashed potatoes, pasta) are safe. After 24 hours, you can resume normal eating.
Avoid very hot or very cold foods and drinks for 48 hours if you experience sensitivity. Temperature extremes stress the tooth during the initial healing period. Room temperature or lukewarm foods and beverages reduce discomfort.
Avoid hard, sticky, or chewy foods (nuts, hard candy, caramel, gum) on the filled tooth for 48 hours. These foods can dislodge a new filling, especially if the filling is large or the tooth structure is weak.
Resume normal brushing and flossing immediately, clean teeth heal faster and maintain better long-term filling integrity. Some patients avoid brushing the filled tooth out of fear, but this causes plaque buildup and increases decay risk around the filling margins.
Normal sensitivity timeline vs warning signs that need a re-check
Mild sensitivity to cold, heat, and sweet foods is normal for 3 to 14 days after a filling. The tooth nerve is temporarily inflamed from the drilling and bonding process, and it needs time to settle. Sensitivity should gradually decrease each day.
- Normal sensitivity characteristics: discomfort lasts 1 to 5 seconds after you remove the trigger; pain is mild to moderate in intensity (you can tolerate it without medication); sensitivity improves steadily over the first week; you can eat and function normally with minor adjustments.
- Warning signs that require re-evaluation: pain that worsens instead of improving after 3 to 5 days; sharp, severe pain when you bite down (indicates high bite or cracked tooth); throbbing pain that keeps you awake at night (indicates nerve inflammation or infection); sensitivity that lasts 30 seconds or more after removing the trigger (indicates possible nerve damage); visible swelling or pus around the tooth (indicates abscess); spontaneous pain without any trigger (indicates irreversible pulpitis).
Contact your dentist if you experience any warning signs. Early intervention often saves the tooth and prevents progression to more complex treatment. At BrightSmile, we reserve appointment slots for post-treatment complications and never charge for simple adjustments within 14 days of the original filling.
Most sensitivity resolves completely within 2 weeks. If you still experience discomfort after 14 days, schedule a follow-up appointment for evaluation. Persistent sensitivity may indicate incomplete decay removal, bonding failure, a crack, or the need for root canal therapy.
Common Problems After a Filling and Kathmandu Cost & Clinic Checklist
Understanding potential complications helps you recognize problems early and seek timely care. This section also provides transparent cost information and a checklist for selecting a reliable dental clinic in Kathmandu.
Pain when biting after a filling: high bite vs deep decay vs crack
The most common complaint after a filling is pain when you bite down, and three main causes exist. High bite (the filling is too tall) is the simplest problem and the easiest to fix. The filling hits the opposing tooth before your other teeth make contact, creating excessive force on one spot. You feel sharp pain during biting that stops immediately when you release pressure. Your dentist adjusts the filling height by grinding down the high spot, and the pain resolves instantly.
Deep decay near the nerve can cause persistent bite sensitivity even after the filling is properly adjusted. The drilling and bacterial toxins inflamed the nerve, and it needs time to heal. This pain usually improves gradually over 7 to 14 days. You can take over-the-counter pain relievers (ibuprofen 400 mg every 6 hours) and avoid chewing hard foods on that side. Pain that worsens instead of improving suggests irreversible nerve damage, and you may need root canal treatment.
A cracked tooth causes sharp, localized pain when you bite down on a specific part of the tooth. The pain stops immediately when you release pressure, similar to high bite pain, but the pain location is very precise, you can identify exactly which cusp hurts. Cracks often occur in teeth with large fillings or in patients who grind their teeth. Your dentist may apply a test (biting on a special device or using transillumination light) to confirm the crack. Treatment options include bonding, onlay, crown, or extraction, depending on crack severity and location.
You should return to your dentist within 48 hours if bite pain does not improve. Delaying adjustment or evaluation allows the problem to worsen and may lead to more extensive treatment.
How long fillings last and when they need replacement (by material)
Filling lifespan varies by material, cavity size, tooth location, and your oral habits. Composite fillings last 5 to 10 years on average. Small fillings in front teeth often exceed 10 years, while large composite fillings in molars may fail within 5 to 7 years due to wear and fracture. Factors that shorten composite lifespan include teeth grinding, heavy bite forces, poor oral hygiene, and high sugar consumption.
Amalgam fillings last 10 to 15 years or longer. Some amalgam fillings placed 20 to 30 years ago are still functional, though the margins may develop secondary decay over time. Amalgam performs best in large, high-stress restorations where composite would fail.
Glass ionomer (GIC) and resin-modified glass ionomer (RMGIC) fillings last 3 to 5 years. These materials are suitable for temporary use, baby teeth, or low-stress areas. We replace them with composite or amalgam once the permanent tooth is fully erupted or the patient can tolerate longer appointments.
Gold inlays and onlays last 15 to 30 years, making them the longest-lasting filling option. Gold does not corrode, resists wear, and tolerates heavy bite forces. The main drawbacks are cost (NPR 40,000 to NPR 80,000 per tooth) and appearance (gold is highly visible).
Porcelain inlays and onlays last 10 to 20 years with proper care. Porcelain matches tooth color beautifully and resists staining, but it can fracture under extreme force. Modern porcelain systems (lithium disilicate, zirconia) are much stronger than older materials.
You should replace a filling when you notice any of these signs: visible cracks or chips in the filling; filling becomes loose or falls out; recurrent decay (dark shadow or cavity) around the filling margins; sensitivity that persists or worsens over time; rough or worn surface that traps food; cosmetic concerns (discoloration, poor color match).
Regular dental check-ups every 6 months allow your dentist to monitor filling integrity and replace worn restorations before they fail completely. Preventive replacement is cheaper and easier than emergency treatment after a filling breaks during a meal.
Filling cost in Kathmandu: what affects price and what’s usually included
Tooth filling costs in Kathmandu range from NPR 1,500 to NPR 6,000 per tooth for direct fillings, depending on material, cavity size, and clinic location. If you want a broader picture of what procedures cost across the city, dental in Kathmandu covers treatment pricing and what to expect from clinics here. Amalgam fillings are the most economical option at NPR 1,500 to NPR 3,000 per tooth. Composite fillings cost NPR 2,000 to NPR 6,000 per tooth, with larger multi-surface fillings toward the upper end. Glass ionomer fillings cost NPR 1,500 to NPR 3,500 per tooth.
Indirect restorations (inlays, onlays, crowns) cost significantly more due to laboratory fabrication and additional appointment time. Porcelain inlay or onlay costs NPR 15,000 to NPR 35,000 per tooth. Full porcelain crown costs NPR 18,000 to NPR 45,000 per tooth. Gold restorations cost NPR 40,000 to NPR 80,000 per tooth, depending on gold market price.
Factors that affect filling cost include cavity size (larger cavities require more material and time), tooth location (front teeth and difficult-to-access areas take longer), material quality (premium composite brands cost more but last longer), dentist experience (specialists may charge higher fees), clinic location (central Kathmandu clinics often charge more than peripheral areas), and whether X-rays and anesthesia are included.
At BrightSmile Dental Clinic, our composite filling package (NPR 2,500 to NPR 5,000 per tooth) includes examination, local anesthesia, X-ray if needed, high-quality composite material, polishing, and bite adjustment. We provide transparent cost estimates before treatment and do not add surprise charges.
Standard filling appointments include examination, X-ray (if not taken recently), local anesthesia, rubber dam isolation (for composite), decay removal, filling placement, shaping and polishing, bite adjustment, and post-treatment instructions. Some clinics charge separately for X-rays (NPR 500 to NPR 1,000 per film) and anesthesia (NPR 300 to NPR 800), so you should confirm what is included in the quoted price.
Most dental clinics in Kathmandu accept cash, eSewa, Khalti, and card payments. We do not typically offer payment plans for simple fillings, but you can arrange installment options for larger treatment plans involving multiple fillings, root canals, or crowns.
Insurance coverage for dental fillings varies by policy. Some health insurance plans in Nepal cover 50 to 70 percent of basic dental treatment, while others exclude dental care entirely. You should contact your insurance provider before treatment to confirm coverage and reimbursement procedures.
Protect Your Smile: Schedule a Check-Up at BrightSmile Dental Clinic
Early cavity detection saves you time, discomfort, and money. We recommend dental check-ups every 6 months to catch decay in the earliest stages, when treatment is simple and conservative.
BrightSmile Dental Clinic in Putalisadak offers comprehensive cavity diagnosis and filling services using high-quality materials and proven techniques. Our new-patient examination package (NPR 1,500) includes a complete oral exam, digital X-rays, professional cleaning (scaling), and a personalized treatment plan, no hidden fees or pressure to accept treatment immediately.
You can book an appointment by calling +977-9748343015, sending a WhatsApp message for a quick cost estimate, or visiting us at Putalisadak, Kathmandu. We maintain strict sterilization protocols, use single-use disposable items wherever possible, and explain every treatment step before we begin.
Our clinic provides same-day emergency appointments for patients with severe tooth pain or broken fillings. We also offer flexible scheduling for working professionals and students who need evening or weekend slots.
Do not wait for cavity pain to force you into treatment. Contact BrightSmile today to protect your dental health with expert, affordable, and patient-friendly care.
How do I know if I have a cavity or just sensitivity?
You may have a cavity if the pain is sharp, localized to one tooth, or triggered by sweets or chewing. Sensitivity from enamel wear or gum recession usually affects multiple teeth and reacts to cold or brushing. A dental exam with X-rays is the most accurate way to confirm the cause.
What are the early symptoms of a cavity?
Early cavity symptoms include white spots, mild cold sensitivity, food getting stuck, or slight discomfort with sweets. Some cavities cause no pain, especially if they develop between teeth. Identifying these signs early can allow remineralization before a filling becomes necessary.
Which tooth filling type is best overall?
The best filling depends on cavity size, tooth location, bite force, and budget. Composite works well for visible areas. Glass ionomer suits gumline cavities and children. Larger molars may need stronger materials like onlays. Dentists recommend based on durability, appearance, and value.
Which filling is best for molars (back teeth)?
The best filling for molars is one that handles high chewing pressure. Composite is suitable for small to medium cavities. Larger cavities may require an onlay or crown for durability. Teeth grinders should choose stronger materials and consider a night guard to prevent damage.
Are silver (amalgam) fillings safe?
Silver amalgam fillings are considered safe and effective. Concerns about mercury exist, but major health organizations support their use. Replacement isn’t needed unless there’s a clinical reason like cracks or leakage. Discuss your personal risk factors with your dentist.
How long do tooth fillings last?
Tooth fillings last 5–15 years depending on material, size, and oral habits. Composite fillings may wear faster if large or exposed to heavy bite pressure. Grinding, poor hygiene, or chewing hard foods can reduce lifespan. Regular checkups detect early damage before it worsens.
Does getting a filling hurt?
Getting a filling usually doesn’t hurt because local anesthesia numbs the area. You may feel pressure or vibration, but not pain. Mild sensitivity after the procedure is normal. If pain worsens or lasts more than a few days, a bite adjustment or recheck may be needed.
When can I eat after a tooth filling?
You can eat after numbness wears off, usually within 1–3 hours. For composite fillings, eat soft foods first. For silver fillings, wait longer before chewing hard foods as they set over time. Avoid eating while numb to prevent biting your cheek or tongue.
Why does my tooth hurt when biting after a filling?
Tooth pain after a filling often comes from a high bite, where the new filling hits too early when chewing. This can cause sharp pain but usually improves with a bite adjustment. Deep cavities may also irritate the nerve. Persistent pain needs evaluation.
When do I need a root canal instead of a filling?
You need a root canal if the nerve is inflamed, infected, or decayed beyond repair. Symptoms include spontaneous pain, lingering sensitivity to hot/cold, or swelling. If the tooth is restorable and pain-free, a filling may be enough. An X-ray confirms the best option.